We’ve been through this before here on The Disease Daily. Our avid readers know that tuberculosis has been around for centuries, though not always by that name: For Hippocrates it was Phthisis, for Europeans in the Middle Ages it was scrofula, and in 18th and 19th century North America it was the grim ‘Captain Among these Men of Death.’ Given such infamy and history, TB is still in our lexicon. But if you were to ask the average inhabitant of a ‘developed’ country to characterize the global TB burden, he or she might have a hard time. We’ve come a very long way to quell TB in wealthy nations, but at the same time have left many less fortunate out in the cold.
For a more details on the history of TB, please refer to this previous Disease Daily article.
According to the CDC, we celebrate World TB Day on March 24 to mark the day when in 1882, Dr. Robert Koch discovered Mycobacterium tuberculosis, the bacillus that causes tuberculosis (TB).”
Although we can cure most cases of TB today, there is a large gap between diagnosis and treatment. The WHO estimates that there will be nearly 9 million new cases of TB this year, but we will not diagnose a staggering 3 million. There is hope. The WHO also estimates 22 million have been reached by the ‘Stop TB’ strategy between 1995 and 2012.
TB is somewhat complicated. You may have heard the terms ‘active’ and ‘latent’ TB. With latent TB, it is possible for an individual to be infected but not exhibit symptoms while the body successfully controls the infection. A person with latent TB is not infectious. A person has ‘TB disease,’ or active TB, once the immune system is unable to fend off the infection. Some people can have latent TB for years, while others, particularly those who are immunocompromised, or have weakened immune systems, may acquire TB disease within weeks of exposure. An individual with TB-infected lungs or throat can spread the bacteria through coughing, sneezing, speaking or singing.
Common symptoms include: a bad cough that lasts three weeks or longer, pain in the chest, coughing up blood or sputum, weakness or fatigue, weight loss, no appetite, chills, fever, and sweating at night.
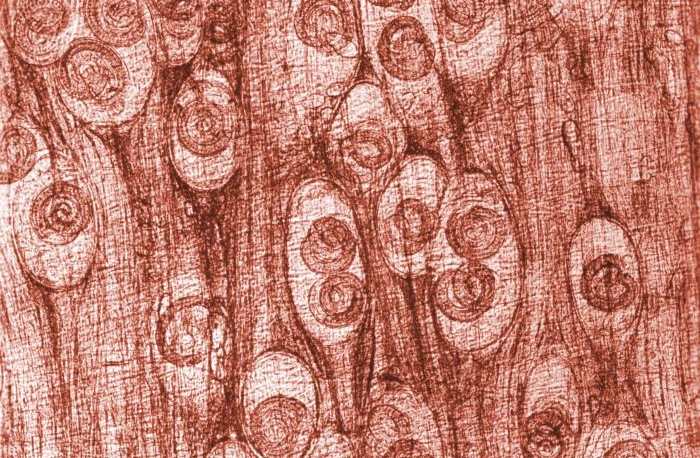
There are various methods to test for TB. Common among developing countries with high TB burden, the ‘sputum smear test’ is widely used. This test, which requires a laboratory, uses a sputum specimen collected from an individual. The sputum is treated with chemicals, which, under a microscope, will stain mycobacteria red. Unfortunately, the test only identifies 60 percent of smear positives (specimens positive for TB infection). Conversely, 40 percent of individuals who are infected with TB will test negative using ‘smear’. These cases are then called ‘false negatives.’ A new highly effective test, called GeneXpert, was adopted to varying extents by 95 countries as of September 2013. GeneXpert, which diagnoses in 2 hours, is highly sensitive. False negative diagnoses are effectively eliminated. It also has the ability to detect drug-resistant TB so that clinicians can immediately tailor appropriate treatment. Drug-resistant tuberculosis is a pretty significant problem. For more, visit previous articles of The Disease Daily. Drawbacks to GeneXpert are largely financial, but as it is a machine, a required central laboratory location also poses difficulty in terms of access to the device.
A number of drug combinations are used to treat latent TB and TB disease. Treating TB typically involves taking a combination of drugs selected from the 10 approved drugs for a period of six to nine months.
An interview with a long-time TB researcher highlights the progress, challenges, and optimism wrapped up in tackling one of the world’s most persistent diseases. C. Robert Horsburgh, Jr., MD, MUS is Professor of Epidemiology, Biostatistics and Medicine and Chairman of the Department of Epidemiology at the Boston University School of Public Health. He has been involved with TB research for over 30 years. I caught up with Dr. Horsburgh in Atlanta after a dual Tuberculosis Trials Consortium (TBTC) meeting and workshop for one of his current clinical trials.
SP: How long have you been conducting TB research and what got you into this field?
RH: Since 1980. As an intern, my first patient was a guy from Jamaica with TB. It was curable and he got better! Very few people were interested in TB at the time, so there weren’t a lot of places to train. I did my infectious disease training at National Jewish in Denver.
SP: What was the greatest accomplishment in the diagnosis and treatment of TB in the past century?
RH: Antibiotics that worked. Development of TB drugs in the 1940s and 1950s led to those scientists winning the Nobel Prize. Sadly, we’ve been able to cure [TB] for 65 years but there’s still a lot of it around so we’re not doing a great job. The ‘theme’ is to find the missing 3 million. WHO estimates there are 8.6 million new cases of TB this year but we won’t find 3 million of them.
SP: What will be the greatest accomplishment in the next 10 years?
RH: Put a dent in cases of TB that aren’t found (and those that are found). There are some new antibiotics coming along but really, there aren’t good diagnostic tools in many parts of the world and [TB] is also stigmatized. There is a lot of stigma. People everywhere are aware that it is stigmatized, but people are in denial. People don’t want to be diagnosed because then the community would know [they’re infected]… and many people aren’t aware it’s curable. They still think it’s a death sentence. Governments like the U.S. need to fund the Global Fund to bring money to countries who can’t find and treat. TB is now a disease of poor countries, though it is still imported to the U.S. It would still benefit everyone to fund.
SP: What about vaccines? Are you optimistic?
RH: There’s a lot of research, but there won’t be a TB vaccine for general use for 5-10 years, at least.
SP: How does the burden of HIV complicate TB treatment?
RH: Global TB burden rose very quickly in the 1990s largely because of HIV before it leveled off. HIV treatment has done a lot to lower TB rates, but HIV infected individuals are still vulnerable. The major problem with TB is that people still aren’t getting diagnosed. In terms of diagnosis, Gene Xpert, being rolled out by the WHO, shows a lot of promise for diagnostic capabilities.
SP: Can you talk about MDR and XDR-TB? Will they be the remnants of the disease in years to come or will they be eliminated in tandem with ‘TB’. What is in the pipeline for treating MDR and XDR TB and do you see these as growing challenges around the world?
RH: Out of an estimated 8.6 million new TB cases around the world, 500,000 are drug resistant, which are much harder to treat. Fewer cures, more deaths. Of these half-million, ¾ never get diagnosed. Of those that do get diagnosed, only 10 percent even get MDR-TB treatment. [Sputum] smear can’t tell if it’s drug resistant, but Gene Xpert CAN tell – so there is promise in the diagnosis.
SP: Any hope for a therapeutic breakthrough? Final thoughts?
RH: We might get a shorter treatment regimen, we might get some new drugs, but nothing that will revolutionize the field. We need better diagnosis and it’s really a failure of political will. We need to send money to poor countries to help with treatment and diagnosis. Of those treated, 87 percent get better, but there are still so many people who don’t know they even have TB. A lot of my efforts have been directed towards treating those with MDR-TB. RESIST-TB is a good resource for people looking for more info. We’re trying to get better treatment regimens and make people aware of the need for better diagnosis. The Zero Declaration movement is also great. People should urge their government to support international TB control and work towards zero TB deaths.
More information from the WHO can be found on their TB page.